|

|
URODYNAMIC
VARIABLES IN A RANDOMISED COMPARISON OF COLPOSUSPENSION AND TENSION-FREE
VAGINAL TAPE (TVT) FOR PRIMARY GSI.
|
|
| |
|
|
|
|
|
|
|
|
| |
|

|
Authors:
|

|
Ward, KL;1 Hilton,
P;1 Browning, J.2 (On behalf of the UK & Ireland TVT trial group)
|
|
| |
|
|
|
|
|
|
|
|
| |
|
|
|
Institution:
|
|
1 University of Newcastle
upon Tyne and the Royal Victoria Infirmary, Newcastle upon Tyne,
England; 2 Ethicon, Edinburgh, Scotland.
|
|
| |
|
|
|
|
|
|
|
|
| |
|
|
|
| |
|
|
|
|
|
|
|
|
| |
|
|
|
|
| |
|
|
|
|
|
|
|
|
| |
|
|
|
|
|
| |
|
|
|
|
|
|
|
|
As a primary procedure for GSI,
colposuspension is generally considered to be the most effective, giving a cure
of up to 85%. (1) An alternative to colposuspension is the TVT (Gynecare, Edinburgh)
with reported cure rates of over 80%.(2) A proportion of women develop new symptoms
following surgery for stress incontinence. These include symptoms of urgency
and urge incontinence. The incidence of detrusor instability (DI) following
colposuspension has been reported to be up to 16%, (3) although the incidence
of urgency symptoms is not well reported. A significant proportion of women
experience delayed voiding following colposuspension, others will have difficulty
voiding long-term.(4) Studies of urethral profile pressures before and after
incontinence surgery show no consistent changes in resting profiles, but enhancement
of pressure transmission following successful procedures.(5)
Aims of study
To evaluate changes in urodynamic variables within the context of a randomised
trial comparing TVT to colposuspension as a primary procedure for genuine stress
incontinence.
Methods
The trial was conducted at 14 centres in the UK and Ireland and included urologists
and gynaecologists, university and district general hospitals. Women with urodynamically
proven GSI were randomised to TVT or colposuspension. None had DI, major voiding
problems, prolapse requiring treatment or previous surgery for incontinence
or prolapse. TVT was performed under local anaesthesia and sedation as described
by Ulmsten.(2) Colposuspension was performed under general or regional anaesthesia.
Assessment performed prior to treatment and at six months post operatively included
symptom and quality of life questionnaires in addition to 1 hour pad test, filling
and voiding cystometry and resting and stress urethral pressure profilometry
by microtransducer (in some centres).
Results
344 patients were recruited to the study and randomised. There were 28 withdrawals
prior to surgery, 23 in the colposuspension group and 5 in the TVT group. 170
underwent TVT and 146 colposuspension, as per protocol. The two groups were
comparable in terms of age, BMI, parity, menopausal status. There was no significant
change in volume at first sensation of filling, cystometric capacity, detrusor
pressure rise on filling or provocation for either procedure. Twelve patients
(7%) in the TVT group and 13 (9%) in the colposuspension group were recorded
as having DI at 6 months post-operatively which was not present pre-operatively.
Overall there was a small reduction in both free flow and catheterised flow,
and a small increase in voiding pressure; this was not significantly different
between procedures. Voiding difficulty was defined as 2 out of 3 of the following:
peak flow <15ml/s; maximum voiding pressure >50cmH2O; residual volume >100ml.
On this basis 6 patients (7%) in each group had voiding difficulty at 6 months
post-operatively (complete data on all these variables was available for only
91 patients in each group). Genuine stress incontinence was recorded during
cystometry in 17 (10%) patients following TVT and 20 (15%) following colposuspension.
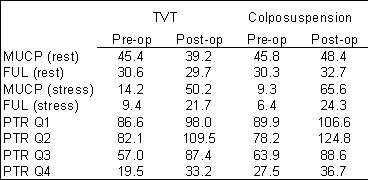
Urethral pressure measurements were available on 48 patients (25 TVT and 23
colposuspension). There no significant changes in resting maximum urethral closure
pressure (MUCP) or functional urethral length (FUL) for either procedure. MUCP
(stress) and FUL (stress) increased for both procedures; this reflects an increase
in pressure transmission ratio (PTR) seen maximally in the second and third
quartiles of the functional urethral length following both operations.
Conclusions
There is a small incidence of both detrusor instability and voiding difficulty
at 6 months following both procedures; this is somewhat lower than previously
reported in respect of colposuspension. Although patients experience less delay
in voiding in the post-operative period following TVT, this is not reflected
in subsequent urodynamic variables. The mechanism of cure following these procedures
appears to be similar; neither is consistently associated with outflow obstruction.
Although the surgical approach in the one case is to the bladder neck, and in
the other to the mid-urethra, the enhancement in PTR is in both cases seen across
the 2nd and 3rd quartiles of the functional urethral length. KW was supported
by a grant from Johnson and Johnson, who also provided materials and additional
support to collaborating centres.
1. BJOG 1994;101(5):371-374.
2. IUGJ & PFD1996;7(2):81-85.
3. BJU 1979;51(3):204-207.
4. O & G 1987;69(1):33-38.
5. BJOG 1983;90(10):934-939.