|

|
TOLTERODINE
IS RAPIDLY EFFECTIVE IN WOMEN WITH MIXED INCONTINENCE
|
|
| |
|
|
|
|
|
|
|
|
| |
|

|
Authors:
|

|
C. Payne 1 and J. Rabin2,
on behalf of the Tolterodine Study Group
|
|
| |
|
|
|
|
|
|
|
|
| |
|
|
|
Institution:
|
|
1 Stanford University
School of Medicine, Stanford, USA
2 Long Island Jewish Medical Center, New York, USA
|
|
| |
|
|
|
|
|
|
|
|
| |
|
|
|
| |
|
|
|
|
|
|
|
|
| |
|
|
|
|
| |
|
|
|
|
|
|
|
|
| |
|
|
|
|
|
| |
|
|
|
|
|
|
|
|
Aims of
Study:
While tolterodine has been shown to be effective in the treatment of overactive
bladder characterised by urge symptomatology, data on its effect in mixed incontinence
is lacking. This prospective, open-label study investigated the efficacy and
tolerability of tolterodine in women with mixed incontinence, urge predominating.
Methods:
135 post-menopausal women aged 50-92 (mean 66) years, recruited on the basis
of urinary urgency, mixed incontinence and urogenital atrophy, were treated
primarily with tolterodine 2 mg twice daily for 16 weeks. Efficacy was assessed
from micturition diaries, collected for 72 hours at 0, 1, 6, 12 and 16 weeks'
treatment, and quality-of-life questionnaires. Tolerability was evaluated from
adverse event reports.
Results:
Changes in endpoint medians from baseline to Weeks 1 and 16, for patients who
completed the study, are shown in the Table below. Statistically significant
changes were seen within 1 week for the symptoms of incontinence, frequency,
volume voided per micturition and pad usage. Figure 1 shows the increase in
dry rate during the study (for patients with incontinence at baseline). This
change is mirrored (Figure 2) by the improvement in the Urogenital Distress
Inventory (UDI) and the Incontinence Impact Questionnaire (IIQ).
| |
Incontinence/24h |
Micturitions/24h |
Vol. voided/micturition
(ml) |
Pads/24h |
| N |
103 |
103 |
103 |
67 |
| Baseline |
2.7 |
10.3 |
164 |
2 |
| Change at Week
1 |
-1.3* |
-1.3* |
+18* |
-0.7* |
| Change at Week
16 |
-2.0* |
-2.0* |
+38* |
-1.0* |
* p<0.0001 vs baseline.
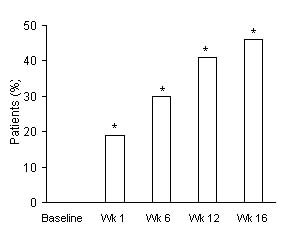
Figure 1. Dry rate
during the study.
*p<0.0001 vs baseline.
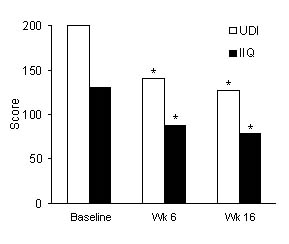
Figure 2. Quality-of-life
improvement.
*p<0.0001 vs baseline.
In patients who
were using pads at study start, there was an overall 50% reduction in pad usage
after 16 weeks' treatment, with 11% (p<0.05) and 30% (p<0.0001) having stopped
usage at Weeks 1 and 12, respectively. Of those who had significant nocturia
(³2 episodes) at baseline, there was a significant reduction in episodes by
study end (p<0.001) with 30% being cured by Week 1 and 35% by Week 16 (both
p<0.0001) [cure was defined as <2 episodes of nocturia]. Quality-of-life measures
improved by 40% for IIQ and by 44% for the UDI (both p<0.0001). Tolterodine
was well tolerated. The most frequent adverse events were dry mouth (33%), headache
(9%) and constipation (7%).
Conclusions:
These findings indicate that tolterodine is rapidly effective in patients with
urinary symptoms of mixed incontinence; all clinical endpoints had significantly
improved by Week 1 and continued to do so to Week 16. The frequency of antimuscarinic
adverse events was low and similar to that reported in other trials. This study
was supported by Pharmacia & Upjohn.